Paper metadata and citation
Title: Understanding Recurrent and Chronic Cystitis. The Role of Diet and Hydration in Different Types and Symptoms of Cystitis
Series: Understanding Recurrent and Chronic Cystitis – White Paper 2
Authors: European Cystitis Observatory (ECO) – Nami Data Intelligence (Erica Ravarelli, Alessio Fabbricatore)
Published: May 2026
Credits and citation
© 2026 Yellow People Lab Srl – Via Privata del Gonfalone 3, 20123 Milano (MI), Italia – P.I. 08594800966
APA: European Cystitis Observatory (ECO). (2026). Understanding Recurrent and Chronic Cystitis – The Role of Diet and Hydration in Different Manifestations of Cystitis (Version V1). Zenodo. https://doi.org/10.5281/zenodo.20125984
Harvard: European Cystitis Observatory (ECO) (2026) «Understanding Recurrent and Chronic Cystitis – The Role of Diet and Hydration in Different Manifestations of Cystitis». Zenodo. doi:10.5281/zenodo.20125984.
Foreword
The relationship between diet and cystitis is one of the most widely discussed topics and, at the same time, one of the least supported by clear evidence in the day-to-day management of the condition. Many people living with recurrent or chronic cystitis spontaneously modify their diet in an attempt to reduce symptoms, often relying on fragmented or research-unvalidated information.
With this white paper, the second in the series "Understanding Recurrent and Chronic Cystitis", the ECO Observatory aims to open new avenues of investigation into the social and behavioural dynamics surrounding cystitis, with the goal of providing concrete impetus for the emergence and development of further studies on the topic.
The analyses presented are based on data collected during the Dimann product assignment process, and were therefore not originally structured with the intent of answering specific research questions. It follows that the results make no claim to exhaustivity: rather, this represents a first exploration of an as yet little-investigated area, conducted with the tools currently available. In this sense, the main value of this work lies in its goal of bringing this topic to the attention of public decision-makers, institutions and researchers, so that they may recognise its potential and the opportunity for new research initiatives.
Executive Summary
Cystitis is one of the most common urological conditions and, when caused by bacterial infection, contributes significantly to overall antibiotic consumption. This has direct implications for the growing spread of antimicrobial resistance, today recognised as one of the leading public health challenges worldwide. The problem takes on even greater significance in recurrent forms of cystitis, which affect a considerable proportion of patients and have a substantial impact on quality of life.
In this context, the search for non-pharmacological preventive strategies and the identification of modifiable lifestyle factors are playing an increasingly central role. Several studies suggest that specific dietary patterns, adequate daily fluid intake and bowel regularity may influence the risk of inflammation, symptom severity and their tendency to recur. These factors are particularly relevant from a clinical standpoint because, unlike many non-modifiable predisposing conditions, they can be addressed through intentional and sustainable lifestyle changes.
Note*relative to symptomatic bacterial cystitis.
Why discuss diet in relation to cystitis?
Diet plays a relevant role in urinary tract health, influencing urine composition, urothelial inflammation and the balance of the urinary and intestinal microbiota. Through metabolites produced by diet and microbiota, nutrients can modulate the chemical environment of the bladder, bacterial growth and the local immune response. Diets rich in fibre, phytonutrients and quality fats appear to support a more stable urinary ecosystem, whereas diets high in refined sugars and saturated fats may promote dysbiosis and inflammation. From this perspective, diet emerges as an important modifiable factor in the prevention and management of cystitis.
In recent years, scientific research has progressively shown that diet does not only affect the domains traditionally associated with nutritional habits, such as general metabolism and cardiovascular health, but also plays a significant role in maintaining the balance and proper functioning of the urinary system. It is now clear that what we eat contributes to shaping the biological environment of the bladder, influencing urine composition, urothelial inflammation and the balance of the urinary microbiota [1]. Diet therefore acts as a kind of biochemical control panel for the urinary ecosystem. Through ingested nutrients, our body produces metabolites that are filtered by the kidneys and eliminated in the urine. These molecules modify fundamental parameters such as urinary pH, the availability of nutrients for bacteria and the inflammatory state of urothelial cells [2]. At the same time, diet profoundly modulates the gut microbiota, which represents one of the main microbial reservoirs from which the bacteria responsible for urinary tract infections can originate [3].
One of the key concepts emerging from the most recent literature is that the intestine acts as a true "microbiological nursery" for many of the bacteria that subsequently colonise the bladder. Numerous uropathogens, including uropathogenic Escherichia coli (UPEC), originate in the intestinal microbiota and can migrate to the urethra and bladder through perineal contamination mechanisms. [1, 2]
In this complex picture, urine represents the final product of the metabolism of ingested food and its chemical composition determines to a large extent which microorganisms can survive and proliferate in the bladder.
Diet therefore plays a fundamental role in determining which bacterial species predominate in the intestine. For example, according to the literature, a diet rich in plant fibre promotes the growth of symbiotic bacteria, such as Bifidobacterium and other beneficial commensals that compete with pathogens for available resources and help reduce the intestinal load of potentially uropathogenic bacteria. Conversely, a Western-style dietary model, characterised by high consumption of refined sugars, saturated fats and low fibre intake, tends to promote conditions of intestinal dysbiosis. In this context, bacterial strains endowed with adhesion structures that facilitate their migration and colonisation of the urinary tract can proliferate. [4]
Also, the quality of dietary fats and the presence of additives typical of ultra-processed foods, such as emulsifiers or artificial sweeteners, can affect the health of the intestinal barrier. Excessive exposure to these compounds can damage the so-called tight junctions between intestinal cells, promoting a condition known as increased intestinal permeability (leaky gut). In this situation, bacterial fragments such as lipopolysaccharides (LPS) and other microbial components can enter the bloodstream or lymphatic system, contributing to a state of systemic inflammation that can also involve pelvic tissues and the bladder.
A further perspective is the classification of foods according to their potential renal acid load (Potential Renal Acid Load, PRAL). Diets characterised by a high PRAL, typically rich in red meat, aged dairy and refined cereals, tend to produce more acidic urine [5]. Although acidity can inhibit certain bacteria, an excessively acidic urinary environment can irritate the nerve endings in the bladder, exacerbating symptoms such as pain, burning and urinary urgency. Conversely, diets rich in fruit, vegetables and legumes generally have a low PRAL and promote the production of citrates and malates, which are excreted as bicarbonates thereby moderately alkalising the urine [5]. Furthermore, a less acidic urinary environment is often less irritating for an inflamed urothelium and can favour the growth of protective bacteria, such as Lactobacilli [6].
Beyond macronutrients, several bioactive compounds in foods can directly influence the ability of bacteria to adhere to the bladder wall or form biofilms. Among these, polyphenols and anthocyanins found in berries, pomegranate and green tea are of particular interest. Part of these compounds is not completely absorbed in the intestine but is transformed by the microbiota into metabolites that reach the bladder through the renal filtrate. Here they can interfere with bacterial adhesion mechanisms, hindering the anchoring of fimbriae to urothelial cells. A similar mechanism has been observed for D-mannose, a sugar naturally present in various fruits, including apples and peaches. This molecule acts as a kind of "molecular bait": E. coli bacteria preferentially bind to mannose molecules present in urine rather than to receptors on the bladder wall, and are then eliminated through urination [7].
Other nutrients instead help modulate the inflammatory response or local immune defences. Omega-3 fatty acids, found in oily fish and flaxseeds, reduce the production of inflammatory mediators such as prostaglandins, while vitamin D stimulates the synthesis of antimicrobial peptides in the urothelium, such as cathelicidin [8].
Micronutrients such as vitamin A and zinc are also fundamental for maintaining the integrity of the urothelial mucosa and for the production of defensins, molecules that help control the density of the urinary microbiota. The latter, in turn, does not represent an isolated system but a dynamic microbial community influenced by diet and intestinal physiology: under balanced conditions, the urinary microbiota in women is often dominated by Lactobacillus, while in men a more mixed community is observed comprising genera such as Corynebacterium and Streptococcus [8].
Some dietary patterns, however, can alter this balance. Recent studies indicate that diets rich in saturated fats and refined sugars also tend to reduce the diversity of the urinary microbiota (alpha-diversity), favouring colonisation by opportunistic species such as Klebsiella or Proteus. Conversely, regular intake of fermented foods, such as yogurt, kefir or sauerkraut, does not necessarily bring live bacteria to the bladder, but contributes to modulating the intestinal and vaginal microbiota, indirectly reducing the migratory pressure of pathogens towards the urethra [6].
Finally, substances such as caffeine, alcohol, spicy foods and certain food additives can pass through the renal filter and reach the bladder in a relatively intact form [5, 6], exerting a direct irritating action on urothelial cells and stimulating the release of inflammatory mediators, including histamine [4]. Conversely, compounds such as polyphenols, antioxidants and flavonoids (including quercetin, found in foods such as apples and onions) can help stabilise the immune cells involved in the inflammatory response and reduce oxidative damage induced by bacterial infection.
The most recent scientific evidence [8], accumulated between 2020 and 2026, suggests that the ideal diet to support a balanced urinary microbiota should prioritise a few fundamental principles:
- a high intake of soluble fibre, useful for promoting the production of anti-inflammatory metabolites such as butyrate;
- a moderate protein intake, preferably from vegetable or lean sources, to avoid excessive urea load;
- a diet rich in phytonutrients, such as flavonoids and anthocyanins, capable of hindering bacterial adhesion;
- an adequate hydration, essential for diluting urine and promoting the mechanical elimination of pathogens.
The role of proper hydration in cystitis
Proper hydration is one of the simplest and most effective behavioural factors in the prevention and management of cystitis. Adequate fluid intake promotes urine dilution, voiding frequency and the so-called mechanical bacterial "wash-out", limiting bacterial adhesion to the bladder mucosa. It also helps reduce urothelial irritation, maintain the balance of the urinary microbiota and support bowel regularity, all of which contribute to reducing the risk of cystitis recurrence.
Among the modifiable factors influencing urinary tract health, hydration is one of the simplest and most effective interventions in both the prevention and management of cystitis. Drinking adequate amounts of water does not only act as a general support to metabolism, but directly modifies the biochemical and microbiological ecosystem of the bladder, influencing urine concentration, voiding frequency, urothelial integrity and the ability of bacteria to colonise the urinary tract.
To understand this mechanism, it can be helpful to imagine the bladder as a biological reservoir in which bacteria attempt to establish themselves and multiply [6]. The main agent responsible for cystitis, E. coli, possesses specialised protein structures called fimbriae, which function as small molecular "hooks" through which bacteria are able to adhere to the inner wall of the bladder. If urine remains stagnant in the bladder for a long time, these microorganisms have the time needed to multiply rapidly and establish colonisation of the urothelial mucosa [9], with doubling times of approximately 20 minutes.
Conversely, adequate fluid intake radically alters this dynamic. The increase in fluid intake stimulates greater urine production and more frequent urination, generating a continuous flow that exerts a true mechanical "wash-out" [10]. In other words, the passage of liquid helps to detach bacteria that have not yet become firmly attached to the mucosa and to eliminate them through urination, reducing the probability that the infection will develop or consolidate.
Beyond the mechanical effect, hydration also acts through important chemical and metabolic mechanisms. Urine is composed not only of water, but contains a mixture of salts, acids and metabolic waste products [10]. Under conditions of dehydration these substances become highly concentrated: a phenomenon easily recognisable from the darker colour and a stronger odour of the urine.
Highly concentrated urine can be chemically irritating to the bladder mucosa, especially when the urothelium is already inflamed. In these conditions, the high concentration of metabolites can act as a direct irritant, exacerbating typical cystitis symptoms such as burning sensation, pain and urinary urgency. Conversely, proper hydration dilutes these substances, making urine less aggressive to bladder tissue and helping to reduce local inflammatory status. Urine dilution also affects bacterial density and the availability of nutrients for microorganisms. In a larger volume of fluid, bacteria are more dispersed and have a lower likelihood of coming into contact with the bladder wall. At the same time, a more dilute urine is relatively poor in metabolic nutrients, making rapid bacterial proliferation more difficult and giving the immune system the time needed to intervene.
A further benefit of hydration concerns the protection of the glycosaminoglycan (GAG) layer lining the urothelium [11], i.e. the inner lining of the bladder. This layer represents a fundamental barrier against bacterial adhesion and the irritating action of substances present in the urine. When the body is dehydrated, urine becomes more concentrated, acidic and rich in salts. This mixture can have an erosive effect on the bladder mucosa, creating micro-irritations that weaken the protective layer and facilitate bacterial adhesion. Maintaining clear and dilute urine, on the other hand, helps preserve the integrity of this "biological shield", reducing both the risk of bacterial colonisation and the intensity of irritative symptoms.
The importance of hydration becomes particularly evident in recurrent cystitis, a condition in which episodes recur frequently over time. In many cases, even when acute symptoms have resolved, the urinary environment may remain favourable to the persistence of small bacterial foci or rapid recolonisation. Maintaining good long-term hydration contributes to stably modifying the ecosystem of the urinary tract [7], reducing opportunities for bacteria to re-colonise the bladder. Studies on bacterial growth in urine have already shown that voiding frequency and the rate of renal filtration represent fundamental factors in limiting microbial proliferation [9]. Consistently with these observations, the European Association of Urology (EAU) guidelines recommend increasing fluid intake as a first-line behavioural intervention in the prevention of urinary tract infections [7].
Regarding the impact on the urinary microbiota, proper hydration also helps maintain favourable conditions in this regard. Recent studies suggest that less concentrated urine favours the survival of protective commensal bacteria [8], while overly dense urinary environments rich in toxic metabolites may hinder these beneficial species and favour the growth of opportunistic bacteria. Hydration also affects urinary pH, a parameter that conditions microbial growth and the tolerability of urine by the urothelium. As highlighted in several review papers on the physiology of hydration [10], adequate fluid availability contributes to maintaining a more stable chemical balance in the urine and to preserving the health of urothelial tissue.
Hydration also plays a relevant role in the context of the so-called gut–bladder axis [12], an expression used to indicate the set of functional, microbiological and immunological interactions that connect the intestine and the urinary tract. The two districts are indeed closely connected: they share anatomical proximity, part of the sacral nervous control and, above all, a relationship mediated by the intestinal microbiota, which represents one of the main sources of bacteria involved in urinary tract infections. Consequently, conditions that affect intestinal function – such as hydration, transit regularity or microbiota balance – can also have repercussions on the urinary environment and susceptibility to bladder infections [8].
Water is indeed essential for the proper functioning of dietary fibre and for maintaining bowel regularity. If fluid intake is insufficient, even a fibre-rich diet may prove ineffective, since fibre tends to absorb water and slow intestinal transit in the absence of adequate hydration [13]. Chronic constipation is a well-known risk factor for urinary tract infections, as faecal stagnation can promote the proliferation of potentially uropathogenic intestinal bacteria and increase the probability of urinary tract contamination [12]. For this reason, proper hydration also indirectly contributes to cystitis prevention by improving intestinal function. The most recent recommendations suggest that daily fluid requirements can be estimated at approximately 25–35 ml of water per kilogram of body weight [13].
Finally, it is important to emphasise that good hydration does not depend solely on the total amount of water ingested, but also on the distribution of intake throughout the day. Drinking large quantities of water at a single sitting leads to rapid elimination of fluids [13] without ensuring effective tissue hydration. Instead, it is preferable to sip water regularly throughout the day, maintaining a constant flow of fluids that promotes stable urine production.
The role of food intolerances and bowel regularity in cystitis
Scientific evidence indicates that food intolerances and alterations in bowel regularity can influence the risk of cystitis through the mechanisms of the gut–bladder axis. Inflammation of the intestinal mucosa, dysbiosis and increased permeability of the intestinal barrier can promote the proliferation and migration of uropathogenic bacteria towards the urinary tract. At the same time, conditions such as chronic constipation increase intestinal bacterial load and can impede proper bladder emptying, creating an environment conducive to infections.
In the context of growing attention to the interactions between the intestine and the urinary tract, food intolerances and alterations in bowel regularity are attracting growing interest, as they may contribute to altering the balance of the intestinal mucosa, microbiota and inflammatory processes, indirectly favouring conditions predisposing to the development or persistence of urinary tract infections. Intolerated foods can promote inflammation of the intestinal mucosa, alterations in microbiota composition and increased intestinal barrier permeability [12], creating an environment that facilitates bacterial proliferation and the spread of potentially pathogenic microorganisms.
However, it should be noted that, in the case of known food intolerances, individuals reasonably tend to eliminate the problematic foods from their diet. Nevertheless, many studies find that the association with cystitis persists for multiple reasons. Firstly, the intolerance itself represents a signal of a heightened systemic sensitivity of the body, indicative of an intrinsic fragility that goes beyond acute exposure to the food, such as an inflammatory predisposition or heightened immune reactivity [13]. Secondly, dietary elimination may not be complete: it often occurs partially or intermittently, allowing residual exposure that maintains a subclinical state. Furthermore, the discovery of the intolerance may occur after years of prolonged consumption, during which the food has already chronically contributed to alterations of the intestinal barrier and microbiota, with persistent effects on the risk of cystitis [18]. At the same time, dietary modification induced by the elimination of specific foods may introduce secondary nutritional imbalances, such as deficiencies or changes in microbial composition, which in turn indirectly favour the pathogenesis of urinary tract infections.
On the other hand, regarding bowel irregularity, this can increase the bacterial load in the colon and promote faecal stagnation, conditions that increase the likelihood of migration of uropathogenic bacteria towards the urinary tract [15] and may contribute to the appearance or recurrence of infections. Among the intestinal factors most relevant to recurrent cystitis is chronic constipation. When intestinal transit is slowed, faeces stagnate longer in the colon and become a true high-density bacterial reservoir, rich in bacteria and opportunistic microorganisms [16]. This stagnation can have consequences at multiple levels: on one hand, the increased intestinal bacterial load raises the likelihood that potentially uropathogenic bacteria will migrate to the urethra; on the other, the accumulated faecal mass in the rectum can exert mechanical pressure on the bladder [2], interfering with its proper emptying and favouring the persistence of urinary residuals, a condition that facilitates bacterial growth. Furthermore, constipation is often associated with a state of intestinal inflammation and dysbiosis, which can further compromise the intestinal barrier function and favour the spread of pro-inflammatory bacterial components into the systemic circulation.
Among the most relevant functions of the intestine is its role as immune regulator of the entire body, modulating numerous immunological and inflammatory processes that can also influence urinary tract health. A balanced intestinal microbiota produces various bioactive metabolites, including short-chain fatty acids (SCFAs), such as butyrate. These molecules play a key role in regulation of systemic inflammation and maintenance of mucosal integrity [8]. Butyrate, in particular, possesses potent anti-inflammatory and immunomodulatory properties.
When a condition of intestinal dysbiosis develops, the production of these protective metabolites can decrease significantly. The reduction in SCFAs, and in particular butyrate, can render the tissues of the pelvic district — including the bladder — more vulnerable to inflammatory processes, increasing susceptibility to infections and the persistence of urinary symptoms.
The relationship between the intestine and the bladder is not only microbiological or immunological, but also has deep anatomical and neurological roots. During embryonic development, these two organs derive from closely related anatomical structures and maintain partially shared innervation throughout life [17]. The nerves regulating the functioning of the rectum and the bladder both originate from the sacral segment of the spinal cord. This neurological connection can generate a phenomenon known as cross-sensitization [18], i.e. cross-sensitization between the two organs. In practice, when the intestine is irritated or inflamed, nerve signals transmitted to the spinal cord can be interpreted as alarm signals for the bladder as well. This mechanism explains why many people affected by irritable bowel syndrome (IBS) or other inflammatory intestinal conditions also experience urinary symptoms, such as urinary urgency or increased urinary frequency, even in the absence of bladder infection [16, 19]. A further element of connection between the intestine and the bladder is the pelvic floor [12], the set of muscles and supporting structures that keep pelvic organs in position and participate in the control of urination and defecation. When intestinal function is altered, for example in the presence of chronic constipation, these muscles may be subjected to repeated strain during defecation, leading to a state of contraction or muscular hypertonia. An excessively contracted pelvic floor can interfere with proper bladder emptying [12], favouring the presence of post-void urinary residual, a condition that increases the risk of bacterial proliferation and urinary tract infections.
Overall, scientific evidence indicates that urinary tract health is closely linked to the balance of the intestinal ecosystem. For this reason, in the management of recurrent cystitis it is increasingly important to adopt an integrated approach that considers not only the bladder, but also the functioning of the intestine. Promoting good bowel regularity, maintaining a balanced microbiota and identifying any foods that may cause inflammation or intolerance is a fundamental step in reducing the risk of infections and improving the health of the entire pelvic district.
In this perspective, the prevention of cystitis does not concern only the treatment of inflammation when it occurs, but also the maintenance of a physiological balance between the intestine, microbiota, immune system and urinary tract [7], elements that together contribute to the stability of the urogenital ecosystem.
The intestine and bladder are more closely connected than one might think. During embryonic development, they form from adjacent structures and share part of the same neural network, originating from the sacral segment of the spinal cord. For this reason, when the intestine is irritated or inflamed, nerve signals can also involve the bladder: this is the phenomenon of cross-sensitization, which explains why those suffering from irritable bowel syndrome often also experience greater urinary urgency. The pelvic floor, which supports both organs, also plays an important role: if it is too contracted — for example due to constipation — the bladder may empty less effectively, promoting bacterial proliferation.
The Dimann Dataset
The study was conducted using the Dimann dataset, a large collection of surveys spontaneously completed by online purchasers of D-mannose. These questionnaires were designed to support the formulation of personalised product recommendations, collecting information on aspects such as habits, individual characteristics, perceived needs and contexts of use. This approach confers a high informational value on the dataset and makes it particularly suited to serve as a solid empirical basis for developing targeted, evidence-based preventive strategies.
The sample analysed comprises over 34,000 anonymised questionnaires, compiled in the period between January 2022 and May 2025. Currently, the dataset is focused on four main European countries — Italy, France, Germany and Spain — offering a relevant comparative overview within different but comparable contexts. In a perspective of continuous development, an extension of the dataset and related analyses is already underway within the ECO Observatory, with the inclusion of new countries in the coming months. This expansion will allow the geographic and demographic coverage to be broadened, further improving the generalisability of the results and the applicative potential of the evidence obtained, both in the preventive field and in support of future strategic decisions.
| Country | Number of observations | % |
|---|---|---|
| Italy | 32,457 | 94.7% |
| Spain | 1,036 | 3.0% |
| France | 721 | 2.1% |
| Germany | 63 | 0.2% |
The questionnaire, organised into thematic sections, explores key behavioural factors related to cystitis, including personal hygiene, dietary and sexual habits, stress levels and other lifestyle aspects. With over 30 variables dedicated to the impact and consequences of the condition – such as effects on mood, social life and productivity – the dataset sheds light on dimensions of the condition that are often overlooked.
| Gender | Number of observations | % |
|---|---|---|
| Woman | 33,628 | 98.1% |
| Man | 628 | 1.8% |
A marked female predominance emerged in the sample, with 98.1% women compared to less than 2% men. This female predominance is likely related both to the targeting of the products offered by Dimann, primarily aimed at women, and to the strong female prevalence in the incidence of cystitis. The remaining 0.1% selected the "other" category, which was excluded from the models.
Age distribution

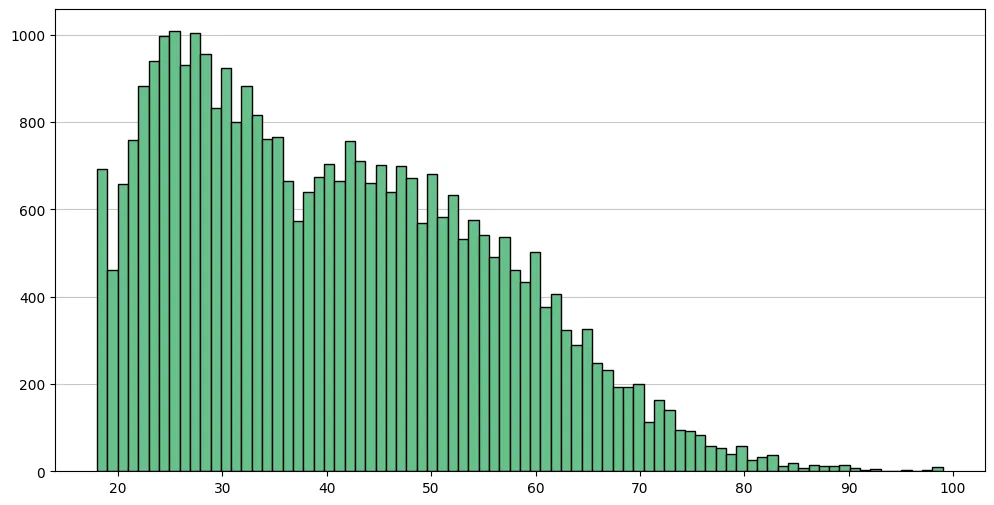
Regarding age, the individuals included in the sample fall within an age range of 18 to 99 years; however, participants over 55 years of age are less represented compared to younger groups. The mean age is 40 years, with a median of 39, indicating a right-skewed distribution. The third quartile, equal to 52 years, shows that 75% of respondents are aged 52 or under. These values suggest that the dataset primarily represents adults in the young and middle-age bracket.
The Dimann Dataset: dietary habits, intolerances and bowel regularity
To systematically analyse the possible role of behavioural and nutritional factors in the modulation of cystitis, the variables included in the study were specifically considered in relation to two central clinical dimensions: the type of the condition and the perceived symptomatology.
The variables relating to dietary regimen, hydration habits, the presence of food intolerances and bowel regularity were therefore treated as indirect indicators of physiological and behavioural contexts that may influence metabolic, intestinal, immune and urinary balance.
In this perspective, each of these dimensions was not analysed as an isolated element, but as part of a system of factors that may contribute to defining specific risk profiles. Dietary habits help define the type of foods consumed daily and their potential impact on inflammation, the intestinal microbiota and urine composition; hydration directly affects urinary dilution and bladder voiding dynamics; food intolerances can influence food choices and the functioning of the digestive system; bowel regularity is a key indicator of gastrointestinal tract balance, known for its interconnections with the urinary system.
In this integrated interpretive framework, behavioural variables can therefore be read as elements potentially associable with specific types of cystitis and different levels of symptom intensity, facilitating the emergence of clinically significant correlations in subsequent analyses. In other words, this approach helps to read daily habits as factors that may help explain why cystitis manifests in different ways and with symptoms of varying intensity, facilitating the identification of clinically useful correlations.
Diet and nutrition
To investigate the dietary habits of people affected by cystitis, including daily water intake and the possible presence of food intolerances, responses to a Dimann questionnaire question about daily nutritional habits were used.
- you do not follow a specific diet;
- you follow a vegetarian diet;
- you follow a vegan diet;
- you follow a paleo diet;
- you follow a macrobiotic diet;
- other.
* Single-answer question
The "other" option in the questionnaire allows participants to manually enter text responses not covered by the predefined options, favouring more detailed and personalised data. During the data preparation and cleaning phase, these textual responses were subjected to a systematic recoding process: the most frequent responses were aggregated into additional categories, enhancing the information collected and more accurately representing actual dietary habits. As a result, three new categories were created, drastically reducing the use of the residual "other" option. This enhanced the descriptive capacity of the variable and the precision of subsequent analyses.
- lactose-free diet;
- gluten-free diet;
- low-carb diet.
The final distribution thus obtained is illustrated in the donut chart in Figure 2. The option "you do not follow a specific diet" emerges as the most frequent response. This category primarily includes omnivorous dietary regimens attributable to an ordinary Mediterranean model, characterised by variety and the absence of formal restrictions or codified dietary structures. The second most common response is vegetarian diet, indicating a significant presence of nutritional choices oriented towards models that differ from traditional omnivorous eating. It should be noted that this option is distinguished from the vegan diet by the inclusion of animal products such as dairy and eggs, while still excluding meat and fish.

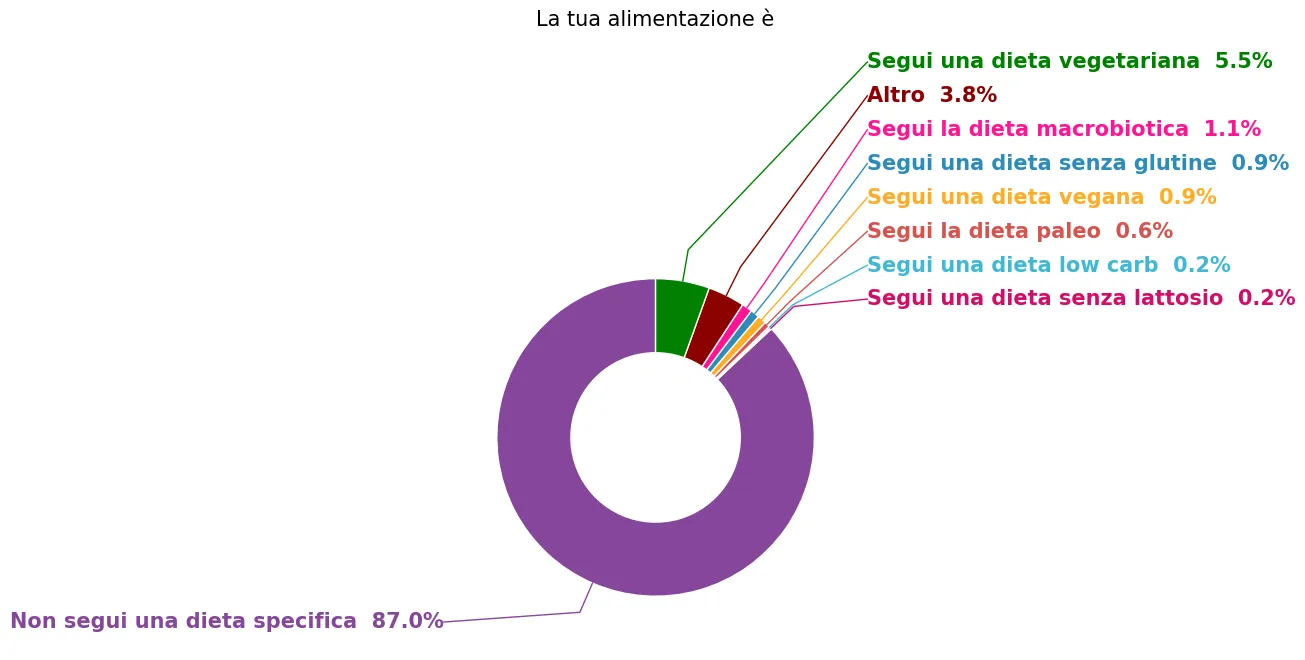
The vegan diet (0.9%), although less frequent than vegetarian (5.5%), highlights a proportion of respondents who adopt a more selective dietary regimen, characterised by the total exclusion of animal products. This figure signals the existence of subgroups with highly structured dietary choices guided by ethical, environmental or health motivations that could influence the incidence and symptomatology of cystitis. The third most frequent category is the macrobiotic diet. This finding is particularly relevant, as it is a structured dietary regimen based on principles of food balance, seasonality and a prevalence of whole grains, vegetables and legumes. Its prevalence in the sample suggests the presence of a subgroup of respondents who adopt dietary choices strongly oriented towards specific and codified nutritional models.
The remaining categories – including gluten-free, paleo, low-carb and lactose-free diets – show progressively lower frequencies. These regimens, often associated with specific needs or targeted nutritional orientations, concern more limited portions of the population considered. Their presence, although minority, is nonetheless relevant from an exploratory analysis perspective, as it may be indicative of particular dietary needs or associated clinical conditions.
Daily water intake
The second key variable analysed is daily water intake, measured through a single-answer question with predefined categorical options. This metric is crucial in discussions relating to cystitis, as adequate hydration promotes urinary flow, reducing bacterial concentration in the bladder and the risk of pathogen adhesion to urethral walls [15]. Similarly to the diet distribution, this variable allows correlation of fluid intake with cystitis type and symptom severity, highlighting potential behavioural influences.
- you have to force yourself to drink;
- one litre or less;
- approximately two litres or more;
- when you have cystitis you drink a lot, when it passes you drink little;
- you don't pay attention.
* Single-answer question
Particularly relevant to the analysis is the presence of the response option "when you have cystitis you drink a lot, when it passes you drink little", which reflects a very common behaviour among patients: increasing fluid intake as a reactive strategy during the acute phase, followed by a reduction in hydration during the asymptomatic phase. This option makes it possible to capture not only the average level of water consumption, but also the behavioural variability linked to the progression of the condition.

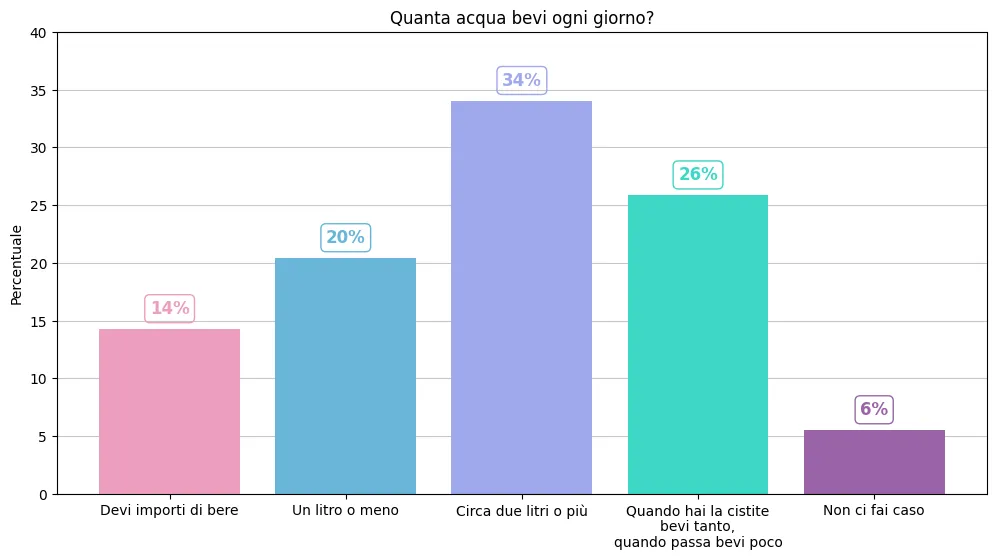
The distribution of responses provides an articulated picture of hydration habits among participants. As shown in Figure 3, the most frequent response is "approximately two litres or more", indicated by 34% of the sample, confirming the presence of a significant proportion of respondents who report water consumption in line with general recommendations. In second place is the option "when you have cystitis you drink a lot, when it passes you drink little", chosen by 26% of respondents. This finding is particularly noteworthy as it highlights a reactive hydration behaviour, closely linked to the appearance of symptoms rather than to a stable daily habit. 20% of respondents report instead drinking "one litre or less" per day, indicating a potentially insufficient level of hydration. In addition to this, 14% report "having to force yourself to drink", signalling a structural difficulty in maintaining adequate fluid intake during the day. Finally, a minority proportion, equal to 6%, states "don't pay attention", highlighting limited awareness of their own water consumption habits.
However, it should be noted that some of these responses do not allow a clear assessment of whether daily fluid intake is actually adequate relative to individual needs. In particular, in the case of "reactive" hydration, fluid intake appears discontinuous and not necessarily sufficient during asymptomatic periods, which actually represent a crucial phase for relapse prevention. Similarly, the responses "have to force yourself to drink" and "don't pay attention" suggest a lack of structure and awareness around hydration habits, making it difficult to establish whether daily intake is in line with recommendations. In these cases, fluid intake may be variable, sporadic or insufficient, without any real monitoring of the quantity consumed.
Overall, this evidence highlights a marked heterogeneity in hydration-related behaviours. The variable as constructed proves useful in distinguishing different consumption profiles, potentially associable with different modes of management and progression of cystitis symptomatology in subsequent analyses.
Food intolerances
A further relevant variable is that concerning food intolerances, which acts as a crucial bridge between nutritional habits, bowel regularity and cystitis dynamics. Alterations of the intestinal microbiota, often induced by intolerances such as lactose or gluten, can promote dysbiosis, increasing intestinal permeability and bacterial translocation towards the urinary tract. Participants were asked the following multiple-answer question (i.e., with the possibility of selecting one or more options).
- no intolerance;
- lactose;
- milk proteins;
- gluten;
- crustaceans;
- other.
Similarly to the approach taken for the dietary regimen variable, in this case too the open-ended responses entered under the "other" category were subjected to a recoding process. Analysis of frequencies made it possible to identify further particularly recurring intolerances, which were converted into independent categories:
- nickel;
- fruit;
- dried fruit/nuts;
- solanaceae;
- yeasts;
- eggs;
- fish;
- medications;
- respiratory allergies;*
- legumes/soya;
- sugars/carbohydrates;
- histamine;
- coffee/cocoa.
This operation made it possible to more fully enhance the information contained in the questionnaire and to reduce the proportion of cases generically classified as "other", improving the descriptive and analytical capacity of the variable. The vast majority of participants – equal to 70% of the sample – report having no specific intolerance. This finding suggests that, for a considerable proportion of people with cystitis, any gastrointestinal disturbances or dietary changes are not linked to diagnosed or perceived intolerance conditions.
Note*Although respiratory allergies do not constitute a food intolerance, it was decided to keep them among the categories analysed as a non-negligible number of participants reported them in the open-ended responses. This inclusion therefore responds to a descriptive criterion and one of completeness in the recoding of spontaneous responses. In subsequent analyses, however, this variable showed no associations or statistically significant results.

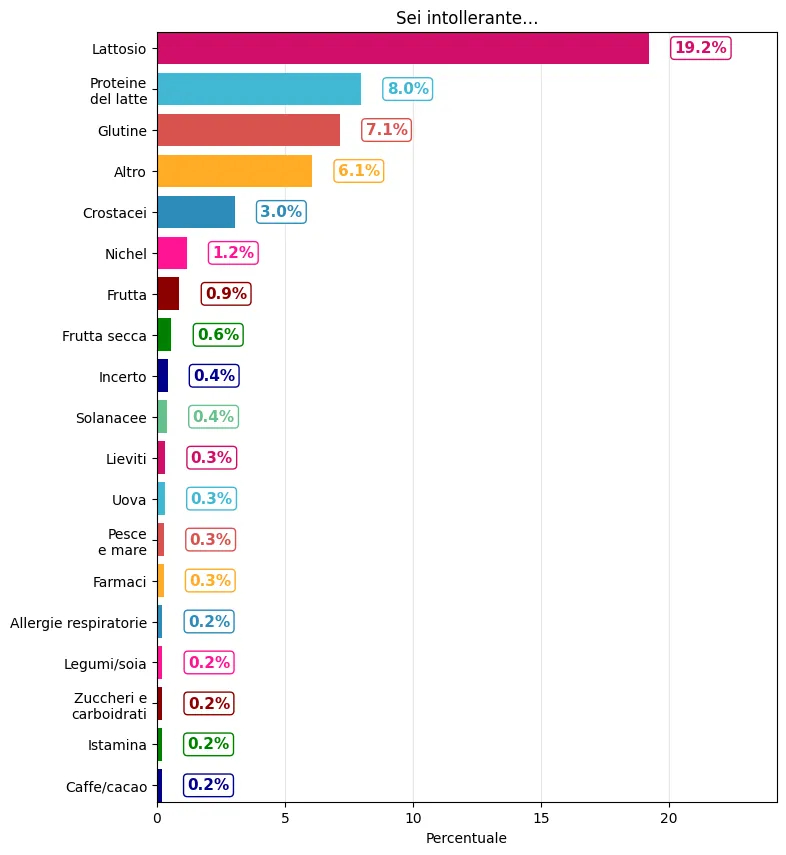
The distribution of responses relating to food intolerances, shown in Figure 4, reveals that, among those reporting at least one intolerance, the most frequent is lactose (19%), followed by intolerance to milk proteins (8%) and gluten (7%). In practical terms, the first two categories refer primarily to the consumption of milk and dairy products: in the case of lactose, a milk sugar, in addition to milk, yogurt, cream, ice cream and various cheeses are often included, while milk protein intolerance is linked to components such as caseins and whey proteins, also present in many industrial preparations where milk or whey may appear among the ingredients. Gluten intolerance, on the other hand, is primarily associated with the cereals that contain it, such as wheat (and related varieties), barley and rye, and therefore products widely consumed such as bread and pasta. Smaller proportions concern intolerance to crustaceans (3%), typically referring to shrimps, scampi, crabs and preparations that include them, followed by more heterogeneous and less frequent conditions, such as sensitivity to nickel (often associated, depending on individual cases, with legumes, cocoa/chocolate, certain vegetables). In the solanaceae category are grouped the intolerances attributed to foods belonging to this family, in particular tomato, potato, pepper and aubergine, in practice also including many everyday derivatives such as tomato passata and sauces, potato-based products or paprika-derived spices. The remaining categories are less represented and more fragmented; among these, at the bottom, residual reports appear such as yeasts, eggs or legumes.
Bowel regularity
Closely connected to food intolerances, a dedicated variable on bowel regularity investigates evacuation frequency. Chronic constipation can in fact alter the intestinal microbiota, favouring the proliferation of uropathogens and their migration to the lower urinary tract.
- every day;
- three to five times per week;
- fewer than three times per week.
* Single-answer question

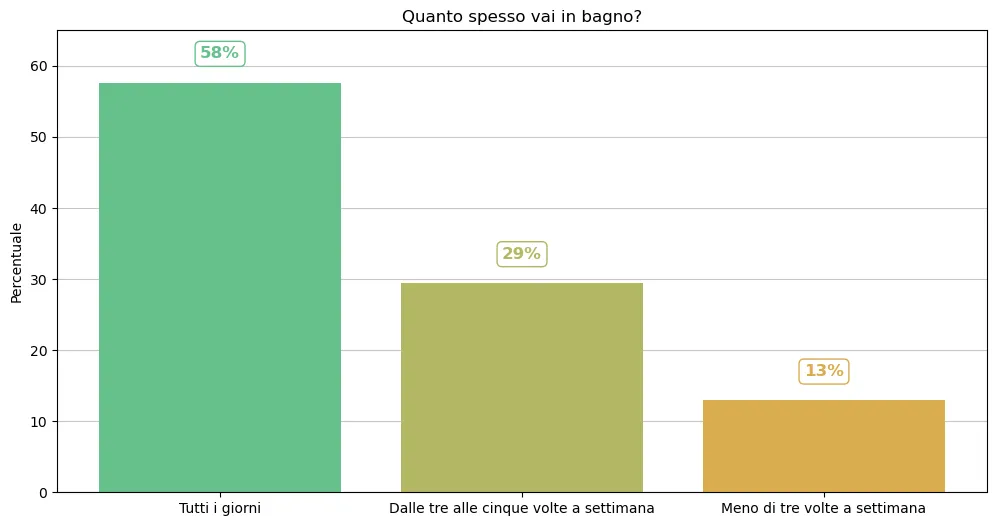
The figure shows that the predominant category is "Every day", selected by 58% of participants, indicating optimal bowel regularity reflecting a balanced microbiota and effective digestive function — both protective factors against dysbiosis and potential bacterial translocation towards the urinary tract. This prevalence suggests the majority of participants enjoy an intestinal function profile that is favourable to reduced cystitis risk. The second most common response, "Three to five times per week" (29%), represents a range still within physiological limits for many adults, but signals suboptimal regularity that could benefit from nutritional optimisation to minimise inflammatory risks. Finally, "Fewer than three times per week" (13%) highlights subclinical constipation in a significant minority, correlated in the medical literature with an altered intestinal barrier, proliferation of uropathogens and an increased incidence of relapses. Overall, over 40% of the sample shows non-ideal regularity, opening opportunities for personalised behavioural interventions such as the integration of prebiotic fibre, specific probiotics or dietary corrections, in synergy with non-antibiotic approaches to the long-term management of the condition.
For detailed information on the procedures adopted, please refer to the Methodological note at the end of this white paper, in which the statistical models implemented are described in detail, together with the data processing criteria and validation procedures.
The Dimann Dataset: cystitis type and symptoms
To assess the impact of the behavioural and nutritional variables examined thus far, we adopted two complementary and fundamental dimensions: the type of the condition and the perceived symptomatology. This multidimensional approach allows a multifaceted and clinically relevant representation of the condition.
The first dimension, cystitis type, classifies the condition based on its clinical presentation: distinguishing, for example, uncomplicated bacterial forms from post-coital, interstitial forms or those associated with anatomical/hormonal factors. This distinction is essential for identifying differential risk patterns. The second dimension, relating to perceived symptomatology, quantifies the intensity of the most common and debilitating symptoms. These include, for example, dysuria, urgency, frequency, pelvic pain and mild incontinence, each of which can be informative of the specific type of cystitis.
The integration of these dimensions generates a disease mapping, not limited to the mere presence of cystitis but extended to its severity and its daily manifestations, enabling precise correlations between behavioural and nutritional risk factors and specific clinical profiles. However, we deliberately excluded episodic frequency, despite it being a key marker for recurrent or chronic cystitis, deferring it to a subsequent dedicated ECO Observatory analysis, in which the impact of dietary habits on inflammation frequency will be explored.
Type of cystitis
To characterise the type of cystitis, a specific single-answer question was used, designed to identify the prevalent form of the condition as identified by respondents.
- cystitis caused by bacteria;
- cystitis triggered by sexual intercourse;
- cystitis without bacteria but with symptoms;
- cystitis that never goes away;
- cystitis with bacteria but without symptoms;
- you don't know.
* Single-answer question
This question makes it possible to capture different clinical manifestations of cystitis as understood and reported by patients. The option "cystitis caused by bacteria" identifies classic infectious forms, generally confirmed by diagnostic tests. The response "cystitis triggered by sexual intercourse" allows the identification of the so-called post-coital cystitis, frequently reported in clinical practice and characterised by specific behavioural risk factors. The option "cystitis without bacteria but with symptoms" captures situations in which symptomatology is present in the absence of infectious evidence, as occurs for example in irritative or interstitial forms. The category "cystitis that never goes away" was included to represent conditions perceived as chronic or persistent, with continuous symptoms over time. The option "with bacteria but without symptoms" finally allows the detection of cases of asymptomatic bacteriuria, while the option "you don't know" allows the identification of respondents who do not have a clear diagnosis or are unable to classify their condition precisely.

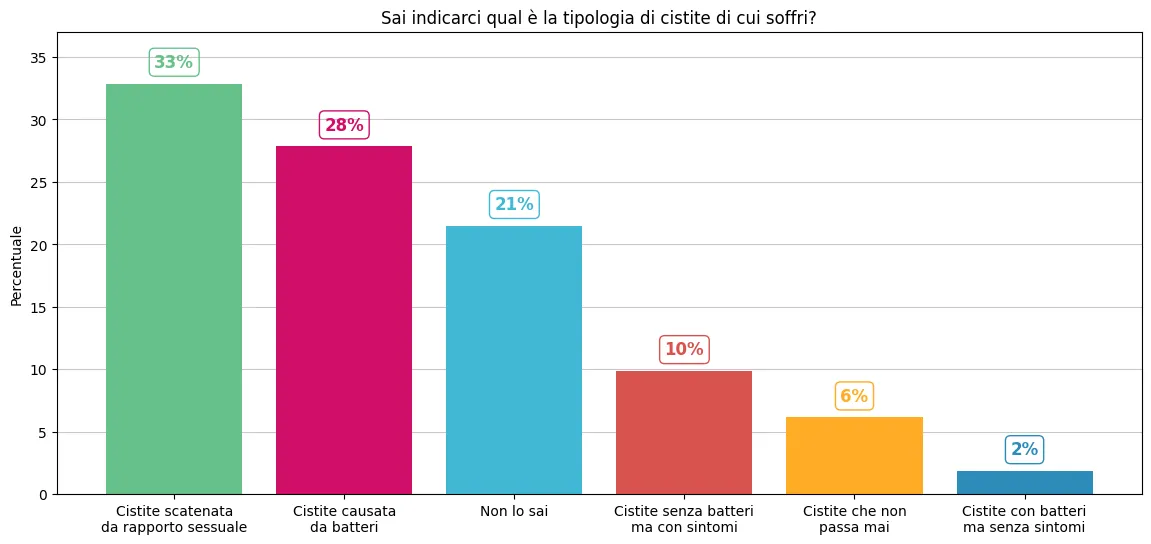
The distribution of cystitis types shows that the most frequent category is cystitis triggered by sexual intercourse, indicated by 33% of the sample. This figure underlines the relevant weight of the mechanical and behavioural factor in the genesis of episodes, confirming that the post-coital dimension represents a central component in the clinical experience of many women. This is followed by cystitis caused by bacteria (28%), which refers to the classic infectious form, generally associated with the proliferation of microorganisms – most frequently E. coli – at the level of the urinary tract. The relevance of this category confirms the presence of a significant proportion of episodes attributable to an infectious aetiology, documented or presumed. This dimension was also explored in the first paper of the ECO Observatory, "Psychological impact of the fight against cystitis. Evidence from Italy", in which the clinical and psychosocial implications of the bacterial forms of the condition were analysed. Smaller proportions concern cystitis without bacteria but with symptoms (10%), which may suggest non-infectious inflammatory pictures or forms similar to interstitial cystitis; cystitis that never goes away (6%), an expression referring to a perception of chronicity or persistence of symptoms; and finally cystitis with bacteria but without symptoms (2%), compatible with pictures of asymptomatic bacteriuria.
Finally, the third most frequent response is "You don't know", indicating that a substantial proportion of respondents report not knowing what type of cystitis they have. This element highlights a possible informational or diagnostic gap, suggesting the presence of clinical pathways that are not always clearly defined or fully understood by patients. Sometimes this lack stems from the diagnostic complexity of cystitis, especially in interstitial or chronic variants where restrictive criteria lead to missed or delayed diagnoses of up to 12 months, with patients often labelled as "psychosomatic".
Cystitis symptoms
Regarding the symptomatology reported by affected women, the question was structured to allow the indication of multiple simultaneous symptoms. Consequently, the sum of percentages does not correspond to 100%, as many women report different combinations of symptoms in the same episode of cystitis.
- Discomfort when urinating
- Fire in the bladder
- Needles and pins
- Chills
- Broken glass in the bladder

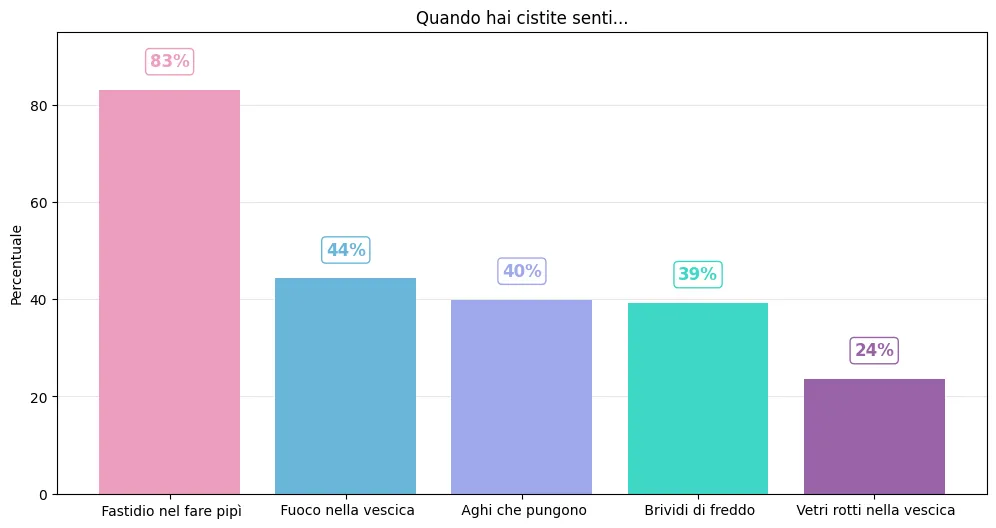
In general, the distribution of symptoms reported by respondents reveals a picture characterised by high perceived intensity and marked heterogeneity in the pain experience. The most frequent symptom by far is "discomfort when urinating" (83%), which represents the most common manifestation, occurring across cystitis episodes. This data confirms that dysuria constitutes the main symptomatological core of the condition, present in the vast majority of cases regardless of clinical type. This is followed by "fire in the bladder" (44%), an expression commonly used by individuals who suffer from cystitis. This symptomatology refers to a sensation of intense, diffuse burning, indicating more marked inflammation of the bladder mucosa. Similar percentages are observed for "needles and pins" (40%) and "chills" (39%). The former describes an acute, punctiform pain, often associated with spasms or bladder overactivity; the latter introduces a systemic dimension to the disorder, suggesting broader inflammatory involvement or a general response of the organism. The symptom "broken glass in the bladder" (24%), although less frequent, represents one of the most evocative and severe descriptions of perceived pain. Its presence in almost a quarter of the sample indicates that a significant proportion of respondents experience episodes with high and potentially debilitating pain intensity.
Results
This section summarises the statistically significant outcomes emerging from the analyses, with the aim of deepening the relationships between the behavioural and nutritional variables considered and the two main clinical dimensions under study: the reported cystitis type and the perceived symptomatology.
In order to isolate the specific contribution of behavioural and nutritional factors, the main objective of the study, the analysis model was integrated with the main available socio-demographic variables, so as to control for any confounding factors. The following sections present the statistically significant results showing the relationships between the behavioural and nutritional variables analysed and the two main clinical dimensions of the study: cystitis type and perceived symptoms.
Type of cystitis
The analyses revealed statistically significant differences between men and women in the presentation of cystitis. In particular, compared to women, men are slightly less likely to report cystitis with bacteria but without symptoms than a symptomatic bacterial form: the relative risk is approximately 9% lower. This suggests that, in comparison with the "classical" bacterial form, the asymptomatic variant is relatively less frequent among men. Conversely, men show an almost twice as high likelihood of reporting cystitis without bacteria but with symptoms compared to the bacterial form, representing the most marked association observed for gender. Regarding post-coital cystitis, men show a relative risk 16.5% higher than women of reporting a form triggered by sexual intercourse compared to the bacterial form. Finally, regarding diagnostic awareness, men are slightly more likely to not know their own type of cystitis (+15% compared to women) relative to the bacterial form.
More nuanced results emerge when considering age. As age increases, a slight reduction in the relative risk of reporting chronic cystitis compared to the bacterial form (-3.4% per additional year). Conversely, age is associated with a significant increase in the relative risk of reporting asymptomatic bacterial cystitis compared to the bacterial form (+36% per unit increase in age, according to the scale used in the model). Finally, consistently with expectations, as age increases the relative likelihood of not knowing one's own type of cystitis also decreases (-27% per additional year of age). This finding can be interpreted as a signal of greater awareness or a greater likelihood of having received a diagnosis over the years.
Turning to the central variables of the study, the presence and type of intolerance show relevant associations with the reported type of cystitis. A first result concerns the theme of convergence between different informational gaps: a significant association emerged between being uncertain about one's intolerance and not knowing the type of cystitis one has. In other words, those who have not investigated their condition in one area have more than double the likelihood (+104.7%) of not having done so in the other. This finding suggests a possible common profile of lower recourse to diagnostic tests or lower clinical awareness. This is therefore not only an association between biological variables, but a coherent behavioural pattern: uncertainty appears to cut across the different health dimensions considered. A particularly interesting result concerns solanaceae intolerance. People reporting this intolerance show an approximately 67% higher likelihood of reporting cystitis without bacteria but with symptoms compared to the bacterial form. Conversely, those reporting this intolerance are slightly less likely (-13%) to report cystitis with bacteria but without symptoms, again in comparison with the bacterial form. Regarding nickel intolerance, a slight increase in the relative risk of reporting chronic cystitis compared to the bacterial form (+2.4%) is observed. This is a statistically significant association, but of limited magnitude.
Other intolerances instead appear to be associated with a lower relative likelihood of certain specific forms. Those reporting fruit intolerance are, for example, much less likely to report cystitis triggered by sexual intercourse compared to the bacterial form (-74%). Tree nut intolerance shows a lower likelihood of reporting cystitis with bacteria but without symptoms (-37% compared to the bacterial form). Overall, these results suggest that intolerances are not simply associated with a general increase or reduction in risk, but rather with a different relative distribution of reported cystitis types.
Regarding the analysis of dietary habits, interesting associations with the reported type of cystitis were identified, although not always homogeneous. Vegetarian and vegan diets are associated with a lower relative likelihood of reporting cystitis triggered by sexual intercourse compared to the bacterial form, meaning the bacterial form is relatively more frequent than the post-coital form. A similar pattern emerges for some restrictive diets in relation to other types. Those who follow a lactose-free diet show a lower likelihood of reporting asymptomatic cystitis (-54%), while for those following a low-carb diet the reduction is more limited (-15%). Similarly, a gluten-free diet is associated with a lower likelihood (-46%) of reporting non-bacterial cystitis compared to the bacterial form. A partially different result is observed instead among vegans regarding the form with bacteria but without symptoms: in this case the relative risk more than doubled compared to those who do not follow a specific diet. Overall, dietary habits do not appear to be associated with a general increase or reduction in risk, but rather with a different relative distribution of cystitis types compared to the bacterial form. Restrictive diets, in particular, appear to be correlated with specific symptomatological profiles rather than a uniform effect.
Regarding the two dimensions of hydration habits and bowel regularity, the analyses did not show statistically significant relationships with the types of cystitis considered. In other words, in the data analysed no systematic pattern emerges linking these behaviours to a greater or lesser relative likelihood of the different forms of inflammation. Although they are variables often cited in clinical and popular debate, no robust associations are observed here that would indicate a differential role compared to the other behavioural and nutritional dimensions analysed. Thus, while diet and intolerances appear to be selectively associated with specific clinical profiles and the distribution of different cystitis types, hydration and bowel regularity do not show significant associations with the classification of the reported form. Conversely, as illustrated in the following paragraph, these dimensions emerge as particularly relevant in the modulation of symptomatology, exerting a more marked influence on the intensity and perception of disorders.
Cystitis symptoms
Moving on to perceived symptomatology, the picture differs markedly from the cystitis type analysis. Here, significant associations emerge between hydration habits, bowel regularity and specific symptoms, such as dysuria and urgency. This suggests distinct mechanisms for the two aspects of cystitis: nutritional factors shape the risk of urinary tract inflammation, while hydration and intestinal function modulate the daily symptom burden, with more immediate effects on perceived wellbeing. Unlike the cystitis type analysis, the evaluation of symptomatology was conducted by treating each symptom as an independent binary outcome, as participants could report multiple manifestations simultaneously. The associations are therefore interpreted as variations in the likelihood of reporting a specific symptom in relation to the variables considered.
Regarding the gender of respondents, a systematic difference emerges in the symptomatology reported by men and women. In all manifestations considered, the male gender is associated with a lower likelihood of reporting a single symptom compared to women. The overall symptom burden analysis confirms this pattern: women report an average of more than two symptoms per episode, while men report fewer than one and a half. Among men the relatively most frequent symptom is "discomfort when urinating", which shows the least marked gap compared to women (-24%). Conversely, the most marked difference is observed for symptoms such as "chills" and "fire in the bladder", for which women show an approximately twice as high likelihood compared to men, suggesting that more intense or systemic manifestations are more frequently reported by the female gender. Overall, these results seem to indicate that men not only report an average lower number of symptoms, but also tend to concentrate more on manifestations that are more "local" and directly related to urination, while women show a more articulate symptomatological profile characterised by a greater presence of painful or systemic symptoms.
Also age shows a systematic association with reported symptomatology. In all manifestations considered, increasing age is associated with a reduction in the likelihood of reporting a single symptom. Although the annual effect is limited (in the order of 1–2.5% per year depending on the symptom), the cumulative impact over larger age intervals becomes relevant. This trend indicates a progressive increase in average symptom burden at more advanced ages.
Moving on to the behavioural and nutritional factors, the analysis of hydration habits yields particularly interesting results in relation to symptomatology. Compared to those who increase fluid intake only during an acute cystitis episode, people who report a constant intake of approximately two litres or more per day show a lower likelihood of reporting "discomfort when urinating" (-19%) and "chills" (-9%), suggesting a possible favourable effect of hydration on some manifestations typically associated with urinary disorders and the systemic component. At the same time, in the same group a slightly higher likelihood of reporting symptoms such as "needles and pins" (+7%) and "broken glass in the bladder" (+11%) is observed, which describe a more localised and punctiform pain component. However, a particularly relevant element emerges when considering the other hydration patterns: compared to the "reactive" group, all other habits are associated with a lower likelihood of reporting the main symptoms analysed, with reductions of between 23% and 34% for manifestations such as "chills" and "discomfort when urinating". This pattern suggests that reactive behaviour does not represent a protective factor, but perhaps rather an indirect indicator of greater symptom intensity. Overall, hydration therefore appears closely connected to symptom management rather than prevention.
Regarding bowel regularity, significant and coherent associations emerge with the hypothesis of a possible worsening of symptomatology in the presence of irregularity. Compared to those who report daily evacuation, people reporting going to the toilet fewer than three times per week show a greater likelihood of reporting certain symptoms, in particular "needles and pins" (+11%) and "chills" (+28%). A similar trend, although of more limited magnitude, is also observed among those who go to the toilet three to five times per week: an increase in the likelihood of reporting "chills" (+13%) and "broken glass in the bladder" (+9%). Overall, the results delineate a possible gradient: as bowel regularity decreases, the likelihood of symptomatic manifestations increases, particularly those that are painful or have a systemic component.
Regarding food intolerances, selective associations emerge with certain symptomatological manifestations. In particular, subjects reporting lactose intolerance show a higher likelihood of reporting painful and localised symptoms: +20% for "discomfort when urinating", +14% for "fire in the bladder" and +17% for "broken glass in the bladder". These are moderate but consistent increases, suggesting an association with greater expression of the non-systemic pain component. Also noteworthy is the finding regarding those who report no intolerance, which shows a greater likelihood only of reporting "discomfort when urinating" (+25%).
Finally, some dietary habits show associations with specific symptomatological manifestations. In particular, those who follow a paleo diet show a lower likelihood of reporting "chills" (-43%), suggesting a lower presence of the systemic component of the disorder. Conversely, among those who follow a vegetarian diet a greater likelihood of reporting the symptom "broken glass in the bladder" is observed (+16%), indicative of a more localised and punctiform pain component. Overall, these results indicate that diet does not appear to uniformly affect the overall symptom burden, but rather on the qualitative mode of symptom expression, contributing to delineating different profiles for specific manifestations.
Highlights
- Results show clear differences between men and women. Men tend to more frequently report cystitis with symptoms but without bacterial infection, and more frequently linked to sexual intercourse. Women, on the other hand, describe episodes with a greater number of symptoms and with more intense or systemic manifestations.
- With advancing age, there is an increased risk of symptomatic non-bacterial cystitis and a general worsening of the reported symptomatological picture. In fact, as age increases, the likelihood of reporting only one symptom decreases.
- People reporting specific food intolerances, such as nickel, solanaceae, fruit and nuts, show different types of cystitis compared to those without intolerances. Furthermore, those intolerant to lactose tend to more frequently report localised pain symptoms. Those who report no intolerance, on the other hand, show a greater likelihood of the most localised and least painful symptom, i.e. discomfort during urination.
- In the observed sample, nutritional factors are more strongly associated with the type of cystitis, while hydration and intestinal function modulate the daily symptom burden, with more immediate effects on perceived wellbeing.
- Vegetarian, vegan, lactose-free and gluten-free diets appear to be correlated with specific inflammation profiles rather than a uniform effect.
- Drinking more does not seem to clearly change the type of cystitis, but may influence symptoms. Those who maintain a constant fluid intake tend to report fewer complaints compared to those who drink a lot only when symptoms appear. However, this association may simply indicate more intense episodes.
- Bowel regularity does not seem to determine the type of cystitis, but is linked to symptom intensity. Those with less regular bowel function tend to more frequently report painful symptoms and more marked manifestations. Overall, as bowel regularity decreases, the likelihood of symptomatic manifestations increases, particularly those that are painful or have a systemic component.
Methodological note
Prior to the analyses, a preliminary data cleaning phase was conducted to ensure the quality and reliability of the sample. In this phase, 30 observations were removed that presented incomplete, inconsistent or manifestly erroneous information. The exclusion mainly concerned questionnaires with missing responses in key variables or with invalid completion patterns. The final dataset used for the analyses therefore consists of N = 34,277 valid observations, selected on the basis of criteria for completeness and consistency of the reported information.
The information collected allows analysis of a broad set of factors potentially associated with the onset and management of cystitis, including dietary habits, hydration levels, bowel regularity, the presence of food intolerances and other lifestyle-related elements. These dimensions are recognised in the literature as relevant components for defining personalised preventive strategies and for reducing the risk of relapse. For the purposes of this study, specific thematic variables were selected, identified in accordance with the analytical objectives and research hypotheses. Among the main thematic variables considered are:
- dietary habits and dietary regimen adopted;
- any food intolerances;
- average daily water intake;
- regularity of bowel movements;
- type and symptomatology of cystitis reported.
These variables were selected as they are considered central to systematically exploring the role of diet and hydration in the management of the condition and its clinical course.
For variables integrated through open-ended responses (dietary habits and intolerances), a recoding activity was also carried out. In particular, textual responses were subjected to a normalisation process, aimed at reducing purely formal differences due, for example, to upper and lower case letters, spelling variations, the presence of accents, punctuation marks or slightly different lexical formulations.
Example: Do you have any food intolerances? Other.
| YES NICKEL |
| Nickel |
| Nickel |
| Intolerant to nickel |
Subsequently, in cases where some open-ended responses contained recurring content clearly attributable to the same substantive meaning, they were aggregated into homogeneous categories. This procedure was applied with particular care to responses that, although expressed freely by respondents, referred to conditions, habits or dietary profiles already observable with a certain frequency in the sample. In such cases, the information was brought back to common classes based on predominant semantic content, so as to avoid excessive fragmentation of the data.
The following control variables also considered relevant to the analysis were included:
- age;
- gender;
- country of residence.
The inclusion of these variables made it possible to take into account possible confounding factors and to improve the robustness of the estimates. In the case of the gender variable, the "other" category, selected by 0.1% of respondents during questionnaire completion, was excluded from the models in order to simplify the interpretation of results, setting the female gender as the reference category and comparing it with the male gender. Furthermore, the extremely small size of this category leads to the conclusion that its exclusion does not entail a loss of relevant information for the purposes of the analysis.
Furthermore, a specific check was conducted by calculating the Variance Inflation Factors (VIF) for the set of regressors considered. The results of the analysis did not reveal any relevant criticalities in this regard. The VIF values observed were in fact limited: the highest value was found for some variables relating to food intolerances (None, lactose). All other coefficients showed lower values, in most cases very close to 1, indicating a very low level of linear association with the other regressors. Regarding the two variables with the highest VIF, the values recorded nevertheless remain within thresholds generally considered acceptable in the literature and not such as to suggest problematic multicollinearity (No intolerance = 4.504795, Intolerant to lactose = 2.815882). Overall, it can therefore be considered that the inclusion of the control variables improved the model specification without compromising the stability and interpretability of the estimates.
The variables analysed are largely categorical or ordinal in nature, as they derive from a structured questionnaire with single-choice or multiple-choice response options from a defined set of options. The main reference categories used in the models were:
- "You do not follow a specific diet" for the variable relating to dietary regimen;
- "When you have cystitis you drink a lot, when it passes you drink little" for the quantity of water intake;
- "Every day" for regularity of bowel movements;
- "Italy" for country of residence;
- "Woman" for the gender variable;
- "Cystitis caused by bacteria" for cystitis type.
For all variables the most frequent category was selected, except for water consumption. In this case, the 'reactive' category was compared with all options that reported specific quantities or indirectly deducible ones, although defined in less precise terms as in the case of the option "have to force yourself to drink".
Regarding food intolerances, participants could indicate more than one option simultaneously. For this reason, each intolerance was treated as an independent binary variable (presence/absence), making it possible to model the possible coexistence of multiple conditions in the same individual. The same approach was adopted for the dependent variable relating to cystitis symptoms, treating each symptom as a dichotomous variable (presence/absence) analysed individually.
For the statistical analysis, logistic regression models were used, selected based on the type of dependent variables considered. In particular:
- to analyse the association between the explanatory variables and cystitis type, a multinomial logistic regression model was estimated, which allows the modelling of categorical outcomes with multiple categories;
- for the analysis of reported symptoms, separate binary logistic regression models were estimated, one for each symptom considered, in order to assess the factors associated with the likelihood of reporting a specific symptom.
The analyses were conducted using the Python language and the statistical libraries pandas, NumPy, SciPy and scikit-learn.
Limitations
As in any investigation based on self-reported data collected through questionnaires, this study also entails certain limitations that must be considered when interpreting the results.
A first limitation concerns the non-probabilistic nature of the sample. The data analysed derive from a questionnaire voluntarily completed by users, potential purchasers of Dimann products, and not from a random sampling design.
A second critical point concerns the uneven distribution of certain socio-demographic variables. In particular, a strong disparity is observed in the frequency of observations between different countries of residence, between genders and between certain age groups. For example, most of the observations come from a limited number of countries and the sample is predominantly composed of female subjects, partly reflecting the higher incidence of the condition in this population but at the same time reducing the possibility of balanced comparisons between groups. Similarly, some age classes are underrepresented, which may limit the precision of the estimates relating to these groups.
A further limitation is linked to the self-reported nature of the information collected. The responses provided by participants may be subject to memory errors, subjective interpretations of the questions or inaccuracies in the classification of their clinical condition. This aspect is particularly relevant in the case of the variable relating to cystitis type, for which a portion of the observations derives from self-diagnosis and not from certified medical diagnosis.
A further critical element concerns the structure of the questionnaire itself. Some questions required the selection of a single response from options that, from a clinical standpoint, are not necessarily mutually exclusive. This may have generated classification errors and produce an excessive simplification of potentially more complex clinical situations.
Further limitations arise from the presence of categories with small sizes in some categorical variables. Some response options are in fact less frequent than others, with a consequent reduction in the statistical precision of the estimates associated with these categories. In some cases, this may make model estimates less stable or limit the ability to identify statistically significant associations.
It should also be considered that the study adopts an observational approach, based on the analysis of associations between variables. Consequently, the results do not allow causal relationships to be established between the factors analysed and the type or manifestation of cystitis symptoms. The relationships observed must therefore be interpreted as statistical associations and not as causal effects.
Finally, although certain relevant control variables were included in the models (such as age, gender and country of residence), it is possible that other unobserved or unretrieved factors from the questionnaire influence the relationships analysed. Variables such as pre-existing medical conditions, pharmacological therapies, genetic factors or other lifestyle components could in fact contribute to explaining part of the variability observed in the data. In light of these limitations, the results of the study must be interpreted with caution. However, the large sample size and the variety of information collected nevertheless allow the identification of patterns and associations of interest that can contribute to understanding the factors associated with cystitis and provide useful indications for future, more in-depth investigations.
Frequently Asked Questions
What is the role of diet in modulating cystitis symptoms?
Diet can influence cystitis symptoms primarily through irritative or protective effects on the bladder mucosa. Certain foods, such as caffeine, alcohol, spicy foods and highly acidic foods, have been associated with a worsening of symptomatology. Conversely, a diet rich in plant-based foods, fibre and omega-3 fatty acids may help modulate the inflammatory response and support the immune system. It is, however, important to highlight that the available evidence is in part heterogeneous and often based on clinical observations rather than randomised controlled trials.
How is the intestinal microbiota involved in the pathogenesis of cystitis?
The intestinal microbiota plays a central role in the pathogenesis of urinary tract infections, as it represents the main reservoir of uropathogenic pathogens, including Escherichia coli. Alterations in microbiota composition (dysbiosis) can promote colonisation and subsequent migration of bacteria to the urinary tract.
This gut-bladder link highlights the importance of strategies aimed at maintaining a balanced microbiota, also from a preventive perspective.
Can constipation be considered a risk factor for cystitis?
Constipation is frequently associated with an increased risk of urinary tract infections, especially in women and children. Reduced intestinal motility can lead to a longer permanence of bacteria in the colon and facilitate their proliferation.
Furthermore, faecal accumulation can exert mechanical pressure on the bladder, interfering with complete urinary emptying and promoting stasis, a further predisposing factor for inflammation.
What nutritional strategies can support intestinal health and reduce the risk of cystitis?
The main strategies include:
- an adequate intake of dietary fibre, which promotes bowel regularity;
- proper hydration, essential for intestinal transit;
- the intake of probiotics, which can contribute to maintaining microbiota balance.
These interventions, if maintained over time, can indirectly reduce the risk of recurrent urinary tract infections or inflammation.
What is the role of probiotics in the prevention of cystitis?
Probiotics are the subject of growing interest in the prevention of urinary tract infections. Certain strains, in particular of the genus Lactobacillus, appear to contribute to restoring a microbial environment unfavourable to colonisation by pathogens [6].
However, clinical evidence is still evolving and does not allow definitive recommendations to be formulated. Probiotics can be considered a support, but not an alternative to standard therapies.
How can sugar consumption influence cystitis?
A high intake of simple sugars can promote bacterial growth and contribute to a state of intestinal dysbiosis. Furthermore, high glucose levels in urine (in pathological conditions) can create an environment conducive to microbial proliferation.
For this reason, moderation of sugar intake is generally recommended, especially in subjects with recurrent infections.
Is it possible to prevent cystitis exclusively through diet and lifestyle?
Diet and lifestyle represent important tools in prevention, but they are not sufficient to guarantee the complete absence of episodes, especially in predisposed subjects.
Effective management of cystitis requires an integrated approach that includes:
- correct hygiene habits;
- adequate hydration;
- balanced diet;
- pharmacological therapy, where indicated.
References
- Worby, C. J., Schreiber, H. L., 4th, Straub, T. J., van Dijk, L. R., Bronson, R. A., Olson, B. S., Pinkner, J. S., Obernuefemann, C. L. P., Muñoz, V. L., Paharik, A. E., Azimzadeh, P. N., Walker, B. J., Desjardins, C. A., Chou, W. C., Bergeron, K., Chapman, S. B., Klim, A., Manson, A. L., Hannan, T. J., Hooton, T. M., … Earl, A. M. (2022). Longitudinal multi-omics analyses link gut microbiome dysbiosis with recurrent urinary tract infections in women. Nature microbiology, 7(5), 630–639. https://doi.org/10.1038/s41564-022-01107-xDoi 10 1038
- Minardi, D., d'Anzeo, G., Cantoro, D., Conti, A., & Muzzonigro, G. (2011). Urinary tract infections in women: etiology and treatment options. International journal of general medicine, 4, 333–343. https://doi.org/10.2147/IJGM.S11767Doi 10 2147
- Magruder, M., Sholi, A.N., Gong, C. et al. Gut uropathogen abundance is a risk factor for development of bacteriuria and urinary tract infection. Nat Commun 10, 5521 (2019). https://doi.org/10.1038/s41467-019-13467-wDoi 10 1038
- Ruța, F., Avram, C., Mardale, E., Maior, R., Filip, C., & Nemeth, S. (2025). Histamine-Producing Intestinal Dysbiosis and Its Role in Lower Urinary Tract Infections and Irritable Bowel Syndrome in Young Women. Nutrients, 18(1), 16. https://doi.org/10.3390/nu18010016Doi 10 3390
- Marinkovic, S. P., Moldwin, R., Gillen, L. M., & Stanton, S. L. (2009). The management of interstitial cystitis or painful bladder syndrome in women. BMJ (Clinical research ed.), 339, b2707. https://doi.org/10.1136/bmj.b2707Doi 10 1136
- Du, Y., Sui, X., Bai, Y., Shi, Z., Liu, B., Zheng, Z., Zhang, Z., Zhao, Y., Wang, J., Zhang, Q., Zhu, Y., Liu, Q., Wang, M., Sun, H., & Shao, C. (2024). Dietary influences on urinary tract infections: unraveling the gut microbiota connection. Food & function, 15(19), 10099–10109. https://doi.org/10.1039/d4fo03271cDoi 10 1039
- EAU Guidelines. Edn. presented at the EAU Annual Congress London, United Kingdom 2026. ISBN 978-94-92671-32-5
- Yang, H.J.; Kim, D.S.; Lee, K.W.; Kim, Y.H. The Urinary Microbiome; Axis Crosstalk and Short-Chain Fatty Acid. Diagnostics 2022, 12, 3119. https://doi.org/10.3390/diagnostics12123119Doi 10 3390
- Hakam, N., Guzman Fuentes, J. L., Nabavizadeh, B., Sudhakar, A., Li, K. D., Nicholas, C., Lui, J., Tahir, P., Jones, C. P., Bent, S., & Breyer, B. N. (2024). Outcomes in Randomized Clinical Trials Testing Changes in Daily Water Intake: A Systematic Review. JAMA network open, 7(11), e2447621. https://doi.org/10.1001/jamanetworkopen.2024.47621Doi 10 1001
- Liska, D., Mah, E., Brisbois, T., Barrios, P. L., Baker, L. B., & Spriet, L. L. (2019). Narrative Review of Hydration and Selected Health Outcomes in the General Population. Nutrients, 11(1), 70. https://doi.org/10.3390/nu11010070Doi 10 3390
- Hurst, R.E., Rhodes, S.W., Adamson, P.B., Parsons, C.L., Roy, J.B. Functional and Structural Characteristics of the Glycosaminoglycans of the Bladder Luminal Surface. The Journal of Urology, Volume 138, Issue 2, 1987, Pages 433-437. https://doi.org/10.1016/S0022-5347(17)43180-6Doi 10 1016
- Scott, A. M., Clark, J., Mar, C. D., & Glasziou, P. (2020). Increased fluid intake to prevent urinary tract infections: systematic review and meta-analysis. The British journal of general practice, 70(692), e200–e207. https://doi.org/10.3399/bjgp20X708125Doi 10 3399
- Fuoco, M. B., Irvine-Bird, K., Curtis, N. J. Multiple sensitivity phenotype in interstitial cystitis/bladder pain syndrome. Can Urol Assoc J. 2014 Nov;8(11-12):E758-61. doi: 10.5489/cuaj.2031.
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary reference values for water. EFSA Journal 2010; 8(3):1459. doi:10.2903/j.efsa.2010.1459. Available online: www.efsa.europa.eu
- Kontiokari, T., Laitinen, J., Järvi, L., Pokka, T., Sundqvist, K., & Uhari, M. (2003). Dietary factors protecting women from urinary tract infection. The American journal of clinical nutrition, 77(3), 600–604. https://doi.org/10.1093/ajcn/77.3.600Doi 10 1093
- Alagiri, M., Chottiner, S., Ratner, V., Slade, D., & Hanno, P. M. (1997). Interstitial cystitis: unexplained associations with other chronic disease and pain syndromes. Urology, 49(5A Suppl), 52–57. https://doi.org/10.1016/s0090-4295(99)80332-xDoi 10 1016
- Panicker, J. N., & Sakakibara, R. (2020). Lower Urinary Tract and Bowel Dysfunction in Neurologic Disease. Continuum (Minneapolis, Minn.), 26(1), 178–199. https://doi.org/10.1212/CON.0000000000000824Doi 10 1212
- Malykhina, A. P. (2007). Neural mechanisms of pelvic organ cross-sensitization. Neuroscience, 149(3), 660–672. https://doi.org/10.1016/j.neuroscience.2007.07.053Doi 10 1016
- Whitehead, W. E., Palsson, O., & Jones, K. R. (2002). Systematic review of the comorbidity of irritable bowel syndrome with other disorders: what are the causes and implications? Gastroenterology, 122(4), 1140–1156. https://doi.org/10.1053/gast.2002.32392Doi 10 1053